In 2026, more women than ever are typing “what is PCOS?” into search bars — not out of curiosity, but out of frustration.
Maybe your periods are unpredictable. Maybe stubborn weight gain won’t budge no matter how clean you eat. Maybe you’ve noticed new facial hair, thinning hair on your scalp, acne that feels teenage all over again — or perhaps none of these, yet something still feels “off.” If you’ve been wondering “what is PCOS in women?” or quietly asking yourself, “how do I know if I have PCOS?” you’re not alone.
Polycystic Ovary Syndrome (PCOS) affects nearly 1 in 10 women worldwide — yet it remains one of the most misunderstood hormonal conditions. And despite its name, PCOS is not just an ovary issue. Modern research now recognizes it as a complex, whole-body endocrine and metabolic disorder that influences hormones, insulin function, inflammation, and even long-term heart health.
For some women, symptoms are obvious — irregular cycles, weight gain, excess facial hair. For others, especially those with Lean PCOS, there may be no outward signs at all, making diagnosis even more confusing. That’s why understanding what’s PCOS goes far beyond a textbook definition. It requires looking at your hormones, genetics, metabolism, and reproductive health together — not in isolation.
In this comprehensive 2026 guide, we’ll break down exactly what PCOS is in medical terms, what symptoms to watch for, how doctors diagnose it, and how to recognize early warning signs — so you can move from confusion to clarity with confidence.

What Does PCOS Stand For?
One of the biggest hurdles for patients is the name itself. PCOS stands for Polycystic Ovary Syndrome, but in the medical community of 2026, there is an ongoing movement to rename it.
The term “Polycystic” is often misleading. When people hear “cysts,” they often think of painful, fluid-filled sacs that might rupture or require surgery. However, in PCOS disease, these are not actually cysts. They are small, immature follicles. In a healthy cycle, several follicles begin to grow, but one eventually becomes dominant and releases an egg (ovulation). In women with PCOS, a hormonal “logjam” occurs; the follicles start to grow but never reach maturity. They remain stalled in the ovaries, appearing on an ultrasound like a “string of pearls.”
Why the name matters for your diagnosis:
- You can have “polycystic” ovaries on an ultrasound and not have the syndrome.
- You can have the syndrome (the hormonal and metabolic issues) and have perfectly “clear” ovaries.
- Searching for “what is PCOS in medical terms” helps clarify that the name describes a potential symptom, not the root cause of the disorder.
What Is PCOS in Medical Terms?
If you were to look at a medical textbook today, PCOS would be defined as a heterogeneous endocrine disorder characterized by hyperandrogenism (high male hormones) and ovulatory dysfunction.
But let’s break that down into plain English. PCOS is a state of hormonal chaos.
- The Endocrine Component: Your ovaries and adrenal glands produce too much testosterone and DHEAS (androgens). While all women need these hormones for bone health and libido, an excess disrupts the delicate communication between the brain and the ovaries.
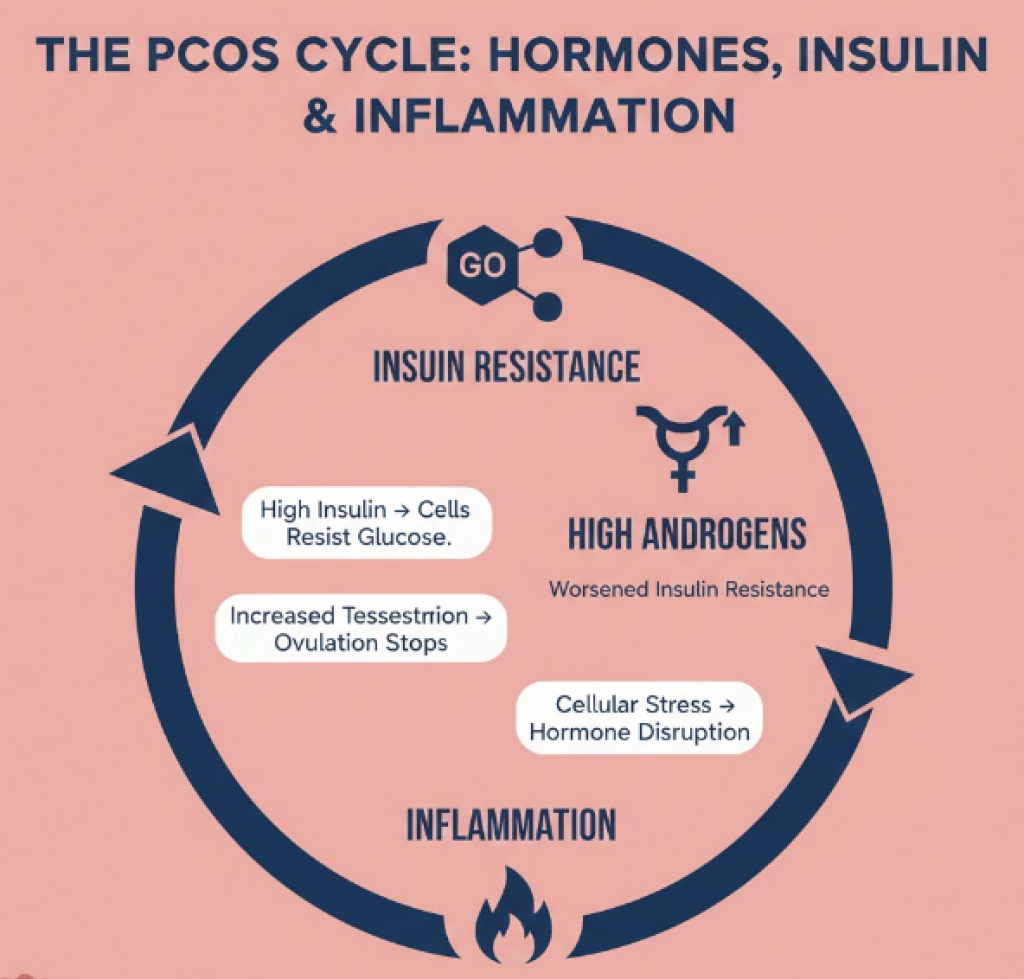
- The Metabolic Component: Most cases are driven by Insulin Resistance. Your body makes insulin, but your cells “ignore” the signal. To compensate, your pancreas produces massive amounts of insulin. This excess insulin is a “mitogen”—it physically stimulates the ovaries to pump out even more testosterone, creating a vicious cycle.
- The Inflammatory Component: 2026 research highlights that what is PCOS is also a state of chronic, low-grade inflammation. This isn’t the kind of inflammation you see with an injury, but a cellular-level stress that contributes to long-term risks like heart disease and diabetes.
Understanding “what is the pcos disease” means realizing it is a systemic condition. It affects your skin, your hair, your mood, and your future metabolic health. It is a lifelong “syndrome” rather than a temporary “illness,” meaning management is about long-term balance rather than a one-time cure.
What Causes PCOS?
When patients ask “how do you get PCOS” or “what causes PCOS in women,” they are often looking for a single culprit, like a virus or a specific dietary choice. However, the scientific consensus in 2026 is that PCOS is caused by a complex “perfect storm” of biological factors. It is not caused by anything you did wrong; rather, it is a mismatch between your genetics and your environment.
The three primary drivers of what is PCOS disease are:
- Insulin Resistance (The Primary Driver): Up to 70% of women with PCOS have cells that are “numb” to insulin. Insulin is the hormone that unlocks your cells to let sugar in for energy. When your cells resist it, your insulin levels skyrocket. This is the “master key” to PCOS because high insulin directly signals the ovaries to overproduce testosterone.
- Androgen Excess (Hyperandrogenism): While often called “male hormones,” androgens are vital for all women. In PCOS, the ovaries produce these in excess. This prevents the follicles from maturing and releasing an egg, which is why what triggers PCOS symptoms like acne and hair growth is almost always a hormonal imbalance.
- Low-Grade Inflammation: Modern research shows that women with PCOS have higher levels of inflammatory markers (like CRP). This chronic inflammation is both a cause and a symptom; it stimulates androgen production and worsens insulin resistance, creating a self-sustaining cycle of hormonal dysfunction.
Is PCOS Genetic? Are You Born With It?
A frequent point of anxiety for many is whether is PCOS genetic or is PCOS hereditary. If you have a mother or sister with the condition, you have a roughly 35% to 50% higher chance of developing it yourself.
- The Genetic Blueprint: There isn’t just one “PCOS gene.” Instead, researchers have identified dozens of small genetic variations related to how your body processes insulin and how your ovaries respond to luteinizing hormone (LH). You are likely born with the predisposition for PCOS.
- The Epigenetic Trigger: Being “born with it” doesn’t always mean you will have symptoms. Often, symptoms are “triggered” by environmental factors. This answers the question: “can you develop PCOS later in life?” While the underlying biology is there from birth, a major life event—like puberty, significant weight changes, or a period of high chronic stress—can “flip the switch” and cause symptoms to emerge.
- When Does PCOS Develop? While it typically becomes evident in the late teens or early 20s (the “classic” onset), many women find that their symptoms only become unmanageable after stopping hormonal birth control, which can mask the signs for years.
What Are Symptoms for PCOS?
To address “how do I know if I have PCOS,” we must categorize the symptoms. Because it is a syndrome, you do not need every symptom to have the condition. In fact, two women with PCOS can have completely different physical experiences.
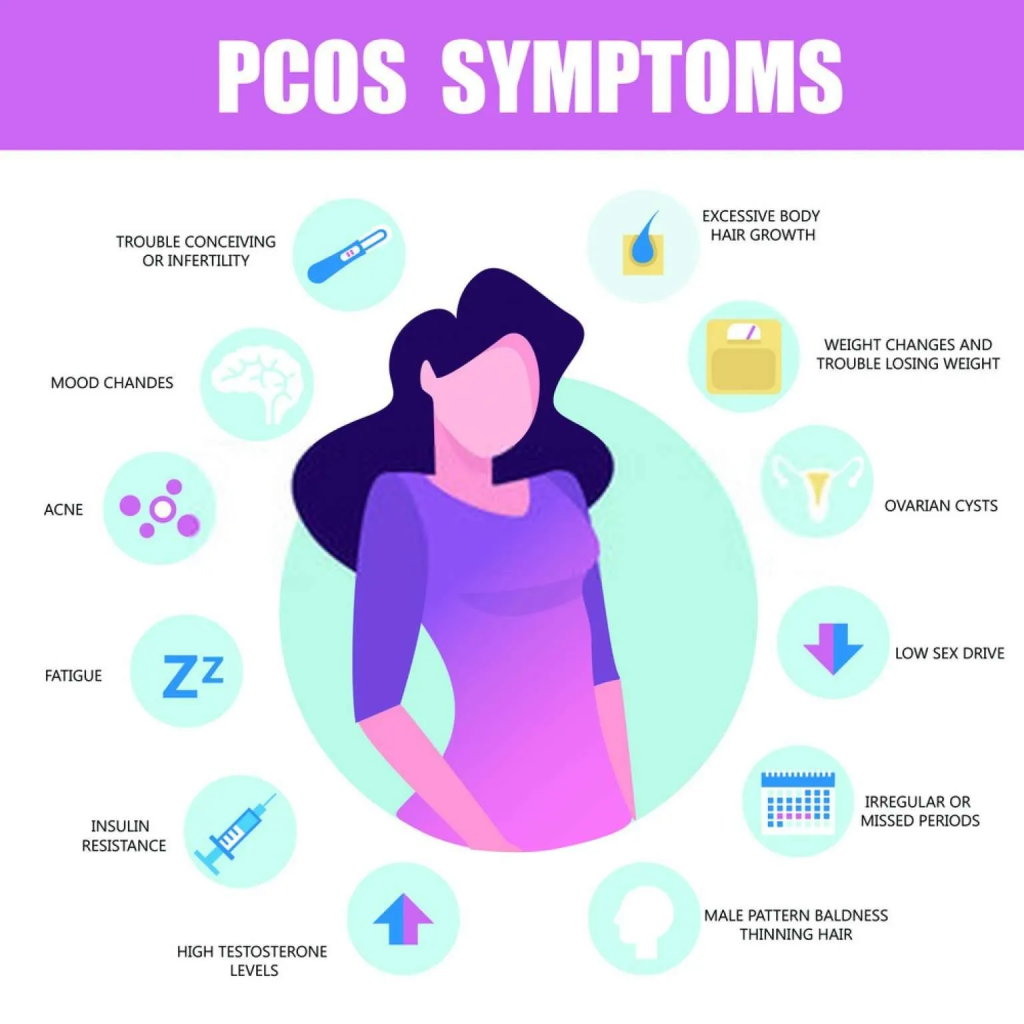
Here are the most common symptoms for PCOS as recognized in 2026:
Menstrual and Reproductive Signs
- Irregular Periods: This is the hallmark. It may mean having fewer than nine periods a year, cycles that are longer than 35 days, or periods that are extremely heavy and painful.
- Anovulation: This is the medical term for not releasing an egg. If you are wondering “can you have PCOS with regular periods,” the answer is yes, but you may still not be ovulating properly (occult anovulation).
Hyperandrogenic Signs (High Testosterone)
- Hirsutism: Excess dark, coarse hair growth on the chin, chest, stomach, or inner thighs.
- Adult Acne: Often severe and concentrated along the jawline and neck.
- Androgenic Alopecia: Thinning of the hair on the top of the scalp, similar to male-pattern baldness.
Metabolic and Systemic Signs
- Weight Gain and “PCOS Belly”: Weight that is specifically difficult to lose and accumulates in the midsection.
- Acanthosis Nigricans: This is a vital how to tell if you have PCOS sign—it involves dark, velvety patches of skin in the folds of the neck, armpits, or groin, indicating high insulin.
- Extreme Fatigue: Often described as “brain fog,” this is linked to the blood sugar “rollercoaster” caused by insulin resistance.
Read more: What Does a PCOS Belly Look Like? Here’s the Entire Picture
Early Warning Signs Most Women Ignore
The early warning signs are often much more subtle. Because PCOS is a spectrum disorder, the body often sends “yellow flags” long before a clinical crisis occurs.
In 2026, medical professionals urge women to look for the following “soft signs”:
- Mid-Cycle Spotting: Often mistaken for a light period, this can actually be a sign of “breakthrough bleeding” caused by a lack of ovulation.
- The “Tired but Wired” Phenomenon: If you experience extreme energy crashes after a high-carb meal followed by insomnia at night, this is a major indicator of the insulin-glucose imbalance central to what is PCOS disease.
- Rapid Hair Greasiness: A sudden increase in scalp oil and skin sebum is often the very first sign that androgen levels are creeping up.
- Persistent Sugar Cravings: This isn’t just a lack of willpower; it is a physiological response to insulin resistance. If you feel you must have sugar to function, your body is likely struggling to manage glucose.
By identifying these early, you can move from wondering “do I have PCOS” to getting a formal evaluation before complications like pre-diabetes or severe hair loss take hold.
Can You Have PCOS Without Cysts?
One of the most frequent points of diagnostic confusion is the belief that you must have cysts on your ovaries to have PCOS. The short answer is: No, you do not need cysts.
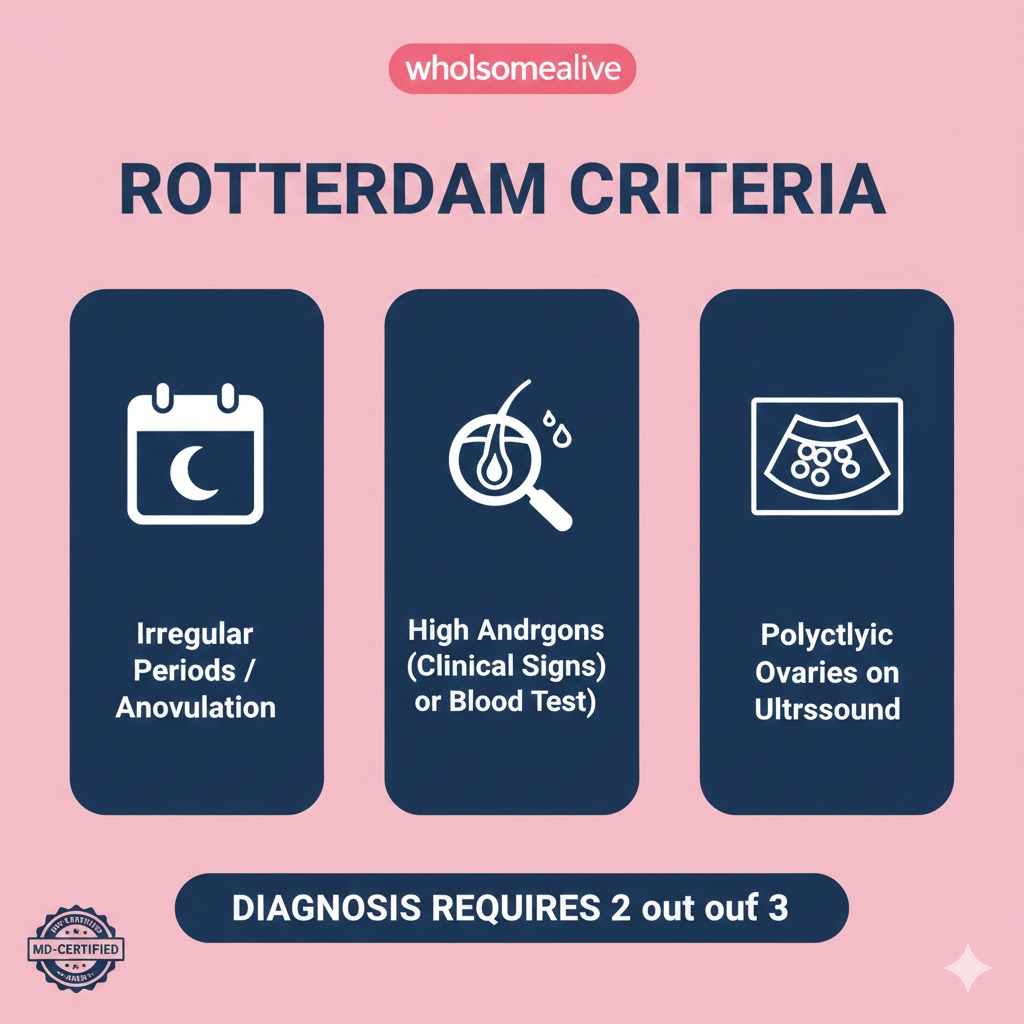
This is why searching for “what is PCOS in medical terms” is so important. Under the globally recognized Rotterdam Criteria, a woman must meet two out of the following three “pillars” to be diagnosed:
- Irregular or Absent Periods (Ovulatory Dysfunction).
- Clinical or Biochemical Signs of High Androgens (Acne, hair growth, or high testosterone in blood work).
- Polycystic Ovaries on Ultrasound (The “string of pearls” appearance).
The Clinical Reality: You can have irregular periods and high testosterone, and even with perfectly “clean” ovaries on an ultrasound, you still officially have PCOS. Conversely, about 20% of women with healthy hormonal profiles have polycystic-looking ovaries, but they do not have the syndrome. This is why a simple ultrasound is never enough to answer “how to test for PCOS”—blood work is non-negotiable.
Can You Have PCOS and Still Have Regular Periods?
A common myth is that a 28-day cycle means your hormones are perfect. This leads many to ask: “can you have PCOS and regular periods?” or “can you have normal periods with pcos?”
The answer is a resounding Yes. This is often seen in what is called “Lean PCOS” (PCOS in women who are at a healthy or low BMI).
- The Regular Cycle Trap: You may have a bleed every month, but you might not be ovulating. This is called an anovulatory cycle. Without a “true” ovulation, your body doesn’t produce enough progesterone, leading to an estrogen-dominant state that still causes hair thinning, mood swings, and “PCOS belly.”
- The “Hidden” Androgen Excess: Some women have very regular periods but suffer from severe cystic acne or hirsutism. If your blood work shows high testosterone or DHEAS, you still meet the diagnostic criteria even if your “period” arrives like clockwork.
- How to Tell: If you have regular periods but are struggling with fertility or androgenic symptoms, a doctor will look for the other two pillars of the Rotterdam Criteria to answer “how to tell if you have pcos.”
Read more: How to Get Periods Immediately in PCOS? Kick-Start Your Periods
How Is PCOS Diagnosed?
If you are wondering “how is PCOS diagnosed”, it is important to know that there is no single “PCOS test.” Diagnosis is a process of inclusion (meeting specific criteria) and exclusion (ruling out other conditions). Because PCOS is a “syndrome,” your doctor must look at the whole picture of your health rather than just one data point.
The modern diagnostic path typically follows this three-step sequence:
- Clinical History: Your doctor will ask detailed questions about your menstrual cycle history. Are your periods “textbook” (28–32 days), or do they vary wildly? They will also look for clinical signs of high androgens, such as persistent adult acne or excess body hair.
- Physical Assessment: This includes measuring your blood pressure, BMI, and waist-to-hip ratio. A key part of how to diagnose PCOS involves checking for physical markers of insulin resistance, such as skin tags or darkened skin patches (acanthosis nigricans).
- The Rotterdam Evaluation: As discussed, your doctor will check if you meet at least two of the three main criteria: irregular periods, high androgens (via blood test or physical signs), and polycystic ovaries (via ultrasound).
If you have irregular periods and visible signs like chin hair, a doctor may technically diagnose you without an ultrasound. However, most 2026 practitioners prefer a full workup to ensure nothing else is being missed.
How to Test for PCOS: Labs and Imaging Explained
To get a definitive answer to “how to test for PCOS,” you will need specific blood work. It is highly recommended to have these tests done in the early morning and, if you still have a cycle, between days 2 and 5 of your period for the most accurate results.
Core Hormone Panel
- Total and Free Testosterone: These are the primary markers for hyperandrogenism. Even if your “Total” is normal, a high “Free” (unbound) testosterone can explain your symptoms.
- DHEAS: This androgen is produced primarily by your adrenal glands. High levels can point to the adrenal-driven subtype of PCOS.
- LH/FSH Ratio: While no longer a strict diagnostic requirement, an LH (Luteinizing Hormone) that is 2 or 3 times higher than your FSH (Follicle-Stimulating Hormone) is a classic “fingerprint” of PCOS.
- Androstenedione: A precursor hormone that can be elevated in women with PCOS.
Metabolic and Blood Sugar Tests
Since insulin is the “engine” of the condition, your diagnostic workup must include:
- Fasting Insulin: This is often the first thing to rise, even if your blood sugar is “normal.”
- HbA1c and Fasting Glucose: To check for pre-diabetes or Type 2 diabetes.
- Lipid Panel: Checking cholesterol and triglycerides, as PCOS significantly increases metabolic risk.
Ultrasound (Imaging)
How to test for PCOS via imaging involves a pelvic ultrasound (often transvaginal). The technician is looking for 12 or more small follicles (2–9mm in diameter) in at least one ovary, or an increased ovarian volume. This provides the “visual” evidence for the “polycystic” part of the name.
PCOS vs. Other Conditions That Mimic It
When PCOS is diagnosed, it is crucial to understand that it is a “diagnosis of exclusion.” This means that before a doctor can officially label you with PCOS, they must prove that your symptoms aren’t being caused by another, similar-looking condition.
In 2026, many women are misdiagnosed with PCOS when they actually have one of the following “mimics”:
- Hypothyroidism: An underactive thyroid can cause irregular periods, weight gain, and thinning hair—symptoms that mirror what is PCOS disease almost perfectly. A simple TSH (Thyroid Stimulating Hormone) test is required to rule this out.
- Hyperprolactinemia: High levels of prolactin (the “milk hormone”) can stop ovulation and cause irregular cycles. This is often caused by a small, benign growth on the pituitary gland, not PCOS.
- Non-Classic Congenital Adrenal Hyperplasia (NCCAH): This is a genetic condition that causes the adrenal glands to overproduce androgens. It looks identical to PCOS on the surface, but it requires different treatment.
- Cushing’s Syndrome: Caused by high cortisol, this can lead to rapid weight gain and facial hair.
PCOS and Mental Health: The Invisible Symptoms
Modern medical guidelines in 2026 have finally recognized that “what is PCOS” isn’t just a physical struggle; it is a mental health struggle. Women with PCOS are significantly more likely to experience anxiety, depression, and eating disorders compared to the general population.
There are three main reasons for this connection:
- Hormonal Fluctuations: High levels of androgens and insulin resistance can interfere with neurotransmitters like serotonin and dopamine, leading to mood instability and “brain fog.”
- Body Image Distress: Symptoms like hirsutism (excess facial hair) and androgenic alopecia (hair thinning) can take a massive toll on self-esteem and gender identity.
- The “Weight Struggle” Stress: Because PCOS causes weight gain that is biologically difficult to lose, many women experience “medical gaslighting” or feelings of failure, which can lead to disordered eating patterns.
Don’t ignore your mental health. If you have the physical signs coupled with unexplained, severe mood swings, it is time to look at the hormonal root cause.
Read more: PCOS Weight Loss Diet and Exercise: Detailed Guide!
Is PCOS Dangerous? Long-Term Health Risks
While PCOS itself is not immediately life-threatening, it is a significant “warning light” for your future health. Because it is a metabolic syndrome, it increases the risk of several serious conditions if left unmanaged.
The primary long-term risks include:
- Type 2 Diabetes: Due to chronic insulin resistance, more than 50% of women with PCOS develop pre-diabetes or diabetes before the age of 40.
- Endometrial Hyperplasia: If you do not have a period for months at a time, the lining of your uterus (the endometrium) can thicken. If this isn’t shed, it increases the risk of endometrial cancer later in life. This is why having at least 4 periods a year is a medical priority.
- Metabolic Syndrome: This is a cluster of conditions including high blood pressure, high blood sugar, and abnormal cholesterol levels, all of which increase the risk of heart disease and stroke.
- Non-Alcoholic Fatty Liver Disease (NAFLD): High insulin levels can cause fat to build up in the liver, even in women who do not drink alcohol.
When Should You See a Doctor?
You should book an appointment if you experience any of the following:
- Menstrual Gaps: You have fewer than 8 periods a year, or your cycles are consistently longer than 35 days.
- Sudden Symptom Flare: A rapid onset of “hormonal” acne or new, coarse hair growth on your face or chin.
- The “Weight Wall”: You are gaining weight (particularly in the abdomen) despite no changes to your diet, or you find it biologically impossible to lose weight.
- Conception Delays: You have been trying to get pregnant for over 12 months (or 6 months if you are over 35) without success.
- Secondary Amenorrhea: Your periods were once regular but have suddenly stopped for 3 months or more (and you aren’t pregnant).
Frequently Asked Questions (FAQ)
1. At what age does PCOS usually start?
PCOS often begins during adolescence, typically within a few years after a girl’s first menstrual cycle. However, many women are not diagnosed until their 20s or 30s, especially if symptoms like irregular periods or acne were previously dismissed as “normal.” Some women only discover they have PCOS when they try to conceive.
2. Can PCOS symptoms suddenly appear later in life?
Yes. While PCOS is considered a lifelong hormonal condition, symptoms can worsen or become more noticeable due to weight gain, stress, insulin resistance progression, or stopping hormonal birth control. Some women only recognize the pattern after coming off the pill.
3. Do all women with PCOS have ovarian cysts?
No. Despite the name “polycystic ovary syndrome,” many women with PCOS do not have visible cysts on ultrasound. The diagnosis depends on a combination of ovulation patterns, androgen levels, and ovarian appearance — not cysts alone.
4. Can you have PCOS if your periods are regular?
Yes. Some women, particularly those with “Lean PCOS,” may have monthly bleeding but still experience hormonal imbalances such as elevated androgens or insulin resistance. Regular periods do not automatically rule out PCOS.
5. Is PCOS only a fertility problem?
No. Although many people associate PCOS with infertility, it is fundamentally a metabolic and endocrine disorder. It increases the risk of insulin resistance, type 2 diabetes, high cholesterol, fatty liver disease, sleep apnea, and cardiovascular disease. Fertility is only one part of the condition.
6. Does PCOS increase the risk of cancer?
PCOS may increase the risk of endometrial (uterine) cancer if irregular ovulation leads to prolonged estrogen exposure without progesterone balance. However, with proper cycle management and medical supervision, this risk can be significantly reduced.
7. Is PCOS the same as being overweight?
No. While weight gain is common due to insulin resistance, PCOS occurs in women of all body sizes. Lean women can have significant hormonal disruption despite a normal BMI. Weight is a symptom modifier — not the cause.
8. Can stress cause PCOS?
Stress alone does not cause PCOS, but chronic stress can worsen hormonal imbalance and insulin resistance, potentially amplifying symptoms in women who are genetically predisposed.
9. Will PCOS go away after menopause?
PCOS does not disappear after menopause. While menstrual irregularities become irrelevant, the metabolic risks — including insulin resistance and cardiovascular risk — may persist and require continued monitoring.
10. Should I see a gynecologist or an endocrinologist for PCOS?
Ideally, both. Gynecologists focus on reproductive symptoms and cycle regulation, while endocrinologists address insulin resistance and metabolic complications. A multidisciplinary approach often provides the best long-term outcomes.
11. Is PCOS curable?
There is no permanent “cure” for PCOS as it is a chronic illness, but it is highly manageable. With the right diet, lifestyle, and medications (like Metformin or GLP-1s), most women can eliminate symptoms and live healthy lives.
References
- World Health Organization (WHO) – Polycystic Ovary Syndrome Fact Sheet
A current global overview of PCOS, including causes, symptoms, and health impact.
https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome - StatPearls – Polycystic Ovarian Syndrome (PCOS)
Free NCBI Bookshelf clinical article summarizing prevalence, diagnosis criteria, and metabolic implications of PCOS.
https://www.ncbi.nlm.nih.gov/books/NBK459251/ - PubMed – Polycystic Ovarian Syndrome (StatPearls Review)
Peer‑reviewed PCOS overview giving diagnostic criteria and associated health risks.
https://pubmed.ncbi.nlm.nih.gov/29083730/ - Endocrine Society Clinical Guideline on PCOS (Diagnosis & Treatment)
Evidence‑based clinical practice guideline with Rotterdam criteria and management recommendations.
https://pubmed.ncbi.nlm.nih.gov/33882124/ - NIH Office of Research on Women’s Health – PCOS Overview
National Institutes of Health resource on PCOS research, genetic factors, and long‑term risks.
https://discoverwhr.nih.gov/research/pcos/