

If you’ve ever asked yourself, “Is PCOS genetic?” or “Are you born with PCOS?” — you’re not alone. These are some of the most searched and emotionally loaded questions about polycystic ovary syndrome. And they make sense. When a condition affects your periods, weight, skin, fertility, and long-term metabolic health, you naturally want to know: Where did this come from?
Many women discover PCOS only after struggling with irregular cycles, difficulty getting pregnant, unexplained weight gain, acne, or excess facial hair. Others may have a mother or sister with the condition and start wondering, “Is PCOS hereditary?” But the answer isn’t as simple as yes or no.
Modern endocrinology no longer views PCOS as just an ovarian issue. It’s a complex, multi-system hormonal and metabolic disorder influenced by genetics, insulin resistance, inflammation, and environmental triggers.
Truth is: you may be born with a predisposition to PCOS, but symptoms often emerge only when certain metabolic or hormonal triggers activate that vulnerability.
In this evidence-based 2026 guide, we’ll break down what research says about PCOS genetics, inheritance patterns, epigenetics, insulin resistance, and why some women develop symptoms in adolescence while others don’t notice problems until their 20s or 30s. By the end, you’ll clearly understand whether PCOS is genetic, whether you’re born with it, and what that actually means for your long-term health.

What Causes PCOS in Women?
One of the biggest frustrations for women is being told “we don’t know exactly what causes it.” While that was true a decade ago, in 2026, we understand that PCOS is a multifactorial endocrine-metabolic disorder. It isn’t caused by one single “glitch,” but rather a perfect storm of five interconnected factors:
A. Insulin Resistance (The Engine)
Up to 80% of PCOS cases are driven by how your body handles insulin. When your cells ignore insulin, your pancreas pumps out more. This “hyperinsulinemia” travels to your ovaries and signals them to produce excess testosterone instead of estrogen.
B. Androgen Excess (The Symptom Driver)
This is the “male-hormone” surge. High androgens prevent your follicles from maturing and releasing an egg (ovulation). Instead, those follicles stay in the ovary as tiny, fluid-filled sacs—what we commonly call “cysts.”
C. Brain–Ovary Signaling Imbalance
Your pituitary gland (the master controller in your brain) produces LH (Luteal Hormone) and FSH (Follicle Stimulating Hormone). In PCOS, the LH is often too high, and the FSH is too low. This “broken telephone” communication means the ovaries never get the clear signal to ovulate.
D. Chronic Low-Grade Inflammation
2026 research confirms that PCOS women have higher levels of inflammatory markers (like CRP). This inflammation isn’t like a fever; it’s a “slow simmer” that damages insulin receptors and keeps the body in a stressed, fat-storing state.
E. Epigenetics
This is the study of how your environment changes how your genes work. You might have the “PCOS gene,” but things like your diet, sleep, and even the environment your mother was in while she was pregnant with you can “turn that gene on.”
Is PCOS Hereditary? What the Research Says
When we ask is pcos hereditary, we have to look at the “Cluster Effect.” If you have PCOS, there is a very high chance that the women (and men) in your family carry metabolic traits that look very similar.
- The Sibling Risk: If you have a sister with PCOS, your risk of having it is roughly 40% higher than the general population.
- Twin Studies: Research on identical twins (who share 100% of their DNA) shows that if one twin has PCOS, the other is extremely likely to have it too, though their symptoms may vary based on their individual lifestyles.
- The Polygenic Nature: There isn’t just one “PCOS Gene.” Instead, researchers have identified over 20 different gene variants that contribute to the condition. Some affect how you process insulin, others affect how your ovaries respond to stress, and some affect your weight distribution.
PCOS tends to run in families, but it doesn’t guarantee you’ll develop it. Think of it like a family trait for high blood pressure or blue eyes — it’s in the deck of cards you were dealt, but how you play the hand matters immensely.
Are You Born With PCOS—Or Does It Develop Later?
This is a nuanced question. In 2026, medical science distinguishes between susceptibility and symptom onset.
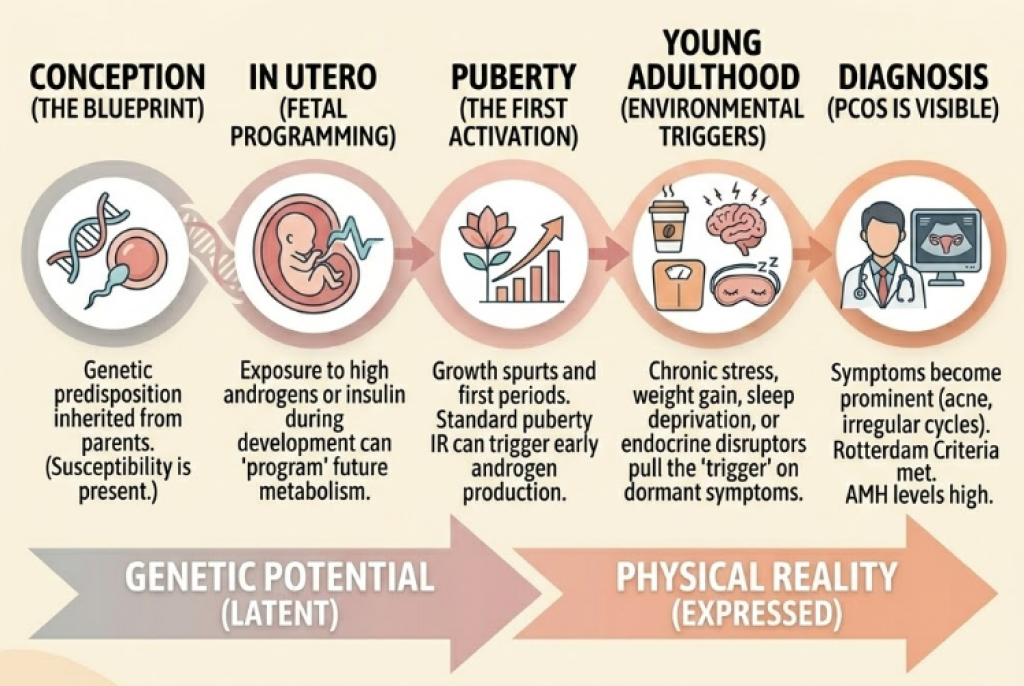
The Susceptibility: Born with it
You are born with the genetic “architecture” for PCOS. New research into Fetal Programming suggests that if your mother had high androgen levels or high insulin while you were in the womb, your “metabolic thermostat” might have been set to a PCOS-prone setting before you even took your first breath.
The Onset: Developing Later
While the potential for PCOS is there from birth, the symptoms almost always require a hormonal catalyst.
- Puberty (The First Wave): For many, the massive hormonal surge of puberty acts as the first trigger. The insulin spike that naturally happens during growth spurts can “kickstart” the androgen production in the ovaries.
- The “Silent” Phase: Some women have the genetics for PCOS but remain symptom-free through their teens because they are active, have low stress, or have high insulin sensitivity.
- The Activation: It is very common to feel like you “developed” PCOS in your 20s or 30s. In reality, a life event (like chronic stress, significant weight gain, or stopping the birth control pill) simply unmasked the condition that was already coded into your DNA.
Can You Develop PCOS Later in Life?
A common story in 2026 fertility clinics is a woman in her late 20s saying, “I never had acne or irregular periods as a teen, so how can I have PCOS now?” This leads many to ask: Can you develop PCOS later in life?
The short answer is: The condition was likely “sleeping,” and life woke it up. While you don’t “catch” PCOS like a cold, several scenarios can cause symptoms to emerge for the first time in adulthood:
- Post-Pill PCOS: Hormonal birth control is a powerful “mask.” It keeps your skin clear and your “periods” (withdrawal bleeds) regular. When you stop the pill to try for a baby, the underlying androgen excess—which was always there—suddenly floods the system.
- The Metabolic Shift: As we age, our natural insulin sensitivity slightly declines. If you had “borderline” PCOS genetics, a 10–15 lb weight gain or a move to a sedentary job can be enough to push your insulin over the threshold, triggering the full syndrome.
- Chronic Stress Onset: High-pressure careers or trauma can spike cortisol. Cortisol and insulin are “metabolic cousins”; when one stays high, the other follows, eventually “switching on” the ovaries’ androgen production.
What Triggers PCOS?
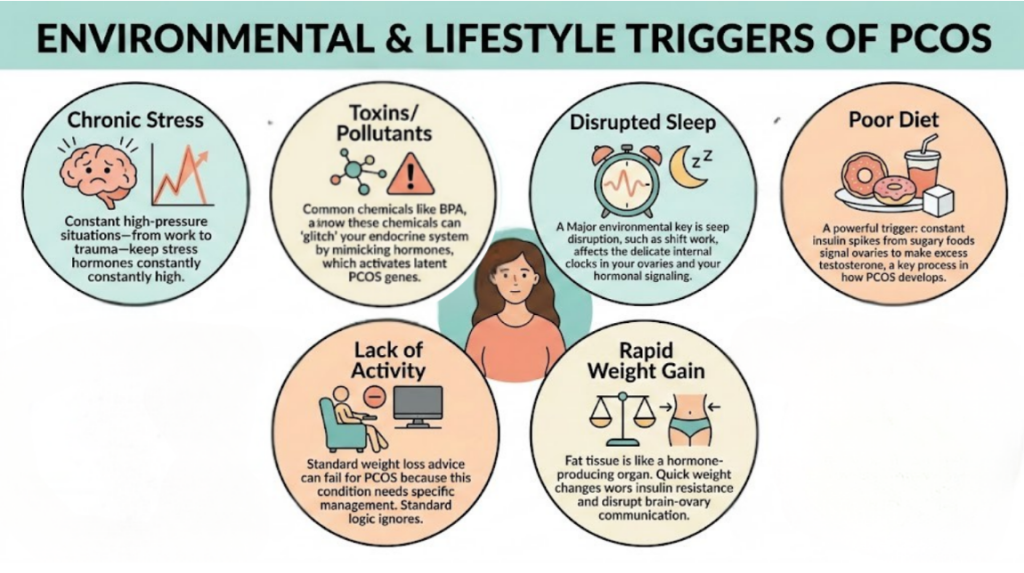
If genetics “load the gun,” these are the triggers that pull it. In 2026, we categorize what triggers PCOS into five distinct environmental pressures:
- Insulin Spikes: Diets high in ultra-processed sugars are the most common triggers. Constant insulin spikes tell the ovaries: “Make more testosterone.”
- Rapid Weight Gain: Fat tissue (adipose) is an endocrine organ. It produces inflammatory signals and estrogen, both of which can disrupt the delicate brain-ovary communication.
- Circadian Disruption: Our ovaries have their own “clocks.” Shift work, blue light exposure at night, and chronic sleep deprivation disrupt the pulsatile release of GnRH (Gonadotropin-releasing hormone), a key player in ovulation.
- Chronic Stress (The Adrenal Trigger): About 20–30% of women with PCOS have “Adrenal PCOS,” where the excess androgens come from the adrenal glands (our stress centers) rather than just the ovaries.
- Endocrine Disruptors (EDCs): We are increasingly looking at BPA, phthalates, and “forever chemicals” (PFAS). These chemicals can mimic hormones and “glitch” the endocrine system, activating latent PCOS genetics.
The Fetal Programming Theory: Can PCOS Start Before Birth?
Utero environment theory suggests that the “seed” of PCOS is planted while you are still a fetus.
- The Androgen Bath: If a pregnant mother has high levels of circulating androgens (testosterone), it can “program” the developing female fetus’s brain and ovaries. It essentially “hard-wires” the baby’s system to be more resistant to insulin and more prone to high LH levels later in life.
- Epigenetic Marking: High insulin levels in the mother can cause “epigenetic tags” to attach to the baby’s DNA. These tags don’t change the gene itself, but they act like a permanent “on switch” for metabolic dysfunction.
Why this matters: It removes the guilt. If your PCOS was “programmed” before you were even born, it proves that this is a biological reality, not a result of “poor choices.”
Why Some Sisters Have PCOS and Others Don’t
If it’s genetic, why does your sister have regular periods and clear skin while you struggle with the full spectrum of symptoms?
- Genetic Recombination: You only share 50% of your DNA with your sister. She may simply not have inherited the same cluster of “PCOS-prone” variants that you did.
- The “Epigenetic Gap”: Even with similar genes, your “lifestyle triggers” might have been different. Perhaps one sister played high-intensity sports (improving insulin sensitivity) during puberty, while the other had a different stress load or diet.
- Different “Faces”: Your sister might actually have the genetics for PCOS but expresses it as “Lean PCOS” (silent or mild symptoms), while you express the “Classic” version.
Does PCOS Come From the Mother or Father?
This is one of the most frequent questions we see in 2026. Because PCOS is an “ovarian” condition, many people assume it only comes from the maternal line. However, genetics are rarely that simple.
The Paternal Connection
You inherit 50% of your DNA from your father, and research has confirmed that men carry PCOS genes. While men obviously cannot have polycystic ovaries, they can pass down the underlying metabolic architecture of the condition.
- The “Male PCOS” Equivalent: Male relatives of women with PCOS often show a specific cluster of symptoms: early-onset male pattern baldness (before age 30), insulin resistance, and a higher risk of Type 2 Diabetes.
- The Inheritance Loop: If your father has a history of metabolic syndrome or early hair thinning, he may have passed the “androgen-sensitive” genetic variants to you. When combined with your female anatomy, those same genes manifest as PCOS.
When Does PCOS Usually Develop?
Timing is everything. While the genetic code is fixed at conception, the expression of PCOS follows a predictable timeline tied to hormonal “surges.”
- The Puberty Peak (Ages 12–15): This is the most common time for onset. The natural “insulin resistance of puberty”—which is normal for growth—can be the final push that triggers androgen excess in genetically predisposed girls.
- The Early Twenties (Ages 20–25): For many, the transition to college or the workforce involves high stress, sleep changes, and different eating habits. This is often when “Silent PCOS” becomes loud.
- The Post-Birth Control Reveal: Many women start birth control at 16 for “acne” and don’t realize they have PCOS until they stop the pill at 28. In these cases, the symptoms didn’t “start” at 28; they were simply unmasked.
Can Birth Control Cause PCOS?
There is a massive amount of misinformation on social media claiming that birth control causes PCOS. Let’s set the record straight for 2026: Birth control does not cause PCOS.
However, it can cause “PCOS Confusion.”
- The Masking Effect: Birth control suppresses your natural hormones and provides synthetic ones that keep your skin clear and your uterine lining thin. It essentially “mutes” PCOS symptoms.
- The “Pill-Induced” Myth: When you stop the pill, your body may experience a “rebound” of androgens as your ovaries wake back up. If your periods don’t return, it’s usually not because the pill caused a new disease—it’s because the pill stopped hiding the PCOS you already had.
Is PCOS Caused by Lifestyle Alone?
If you have ever felt like your PCOS is “your fault” because of what you ate or how much you exercised, please read this carefully: Lifestyle does not cause the root genetics of PCOS.
- The Proof: There are elite athletes and women who eat perfectly “clean” who still struggle with PCOS. There are also people who eat high-sugar diets and have high stress who never develop the condition.
- Lifestyle as a “Dial”: Think of your lifestyle like a volume knob on a radio. The “PCOS Radio” was built into your genetics; your lifestyle choices simply determine how loud the symptoms play.
- The Empowerment Angle: While you didn’t choose your genetics, knowing that lifestyle influences the expression is actually good news. It means you have the power to “turn the volume down” on your symptoms through the strategic changes we discussed in our previous guides.
The Role of Insulin Resistance in PCOS Development
If genetics are the “blueprint,” Insulin Resistance (IR) is the construction crew that builds the PCOS symptoms. To truly understand how do you get PCOS, you have to understand the metabolic domino effect.
- Hyperinsulinemia: Because of your genetics, your cells are “stubborn.” Your pancreas overproduces insulin to compensate.
- Theca Cell Stimulation: These are specific cells in your ovaries. High levels of insulin act like a megaphone, telling these cells to churn out testosterone.
- Follicular Arrest: This flood of testosterone prevents your eggs from reaching maturity. Instead of one egg being released (ovulation), dozens of small follicles get “stuck,” leading to the classic polycystic appearance on an ultrasound.
- The “Sugar-Hormone” Feedback Loop: The more testosterone you produce, the more visceral (belly) fat you store. That fat then produces inflammatory markers that make your cells even more resistant to insulin.
Can PCOS Be Prevented If It’s Genetic?
In 2026, we don’t talk about “preventing” the genes, but we do talk about preventing the expression. If you know PCOS runs in your family, you can take steps to keep the “gun” from being triggered.
- Early Metabolic Screening: If you have a daughter, monitoring her insulin sensitivity during the onset of puberty can change her life.
- The “Stable Weight” Strategy: Preventing rapid weight fluctuations during hormonal shifts (like starting college or changing careers) can keep PCOS symptoms in a “silent” state.
- Sleep Hygiene: Since circadian disruption is a major trigger, protecting your sleep in your late teens and early 20s is one of the most effective ways to manage your genetic risk.
How Is PCOS Diagnosed?
Diagnosis isn’t just about one blood test. To be officially diagnosed, most doctors use the Rotterdam Criteria, which requires two out of the following three:
- Irregular Periods (Oligo-ovulation): Cycles longer than 35 days or having fewer than 9 periods a year.
- Clinical or Biochemical Androgen Excess: This means either physical symptoms (acne, hair thinning, hirsutism) OR high testosterone/DHEAS levels in your bloodwork.
- Polycystic Ovaries on Ultrasound: The presence of 12 or more small follicles on one or both ovaries.
Doctors are now placing higher value on Anti-Müllerian Hormone (AMH) levels as a marker for PCOS, as it’s often significantly higher in women with the condition.
FAQ:
Can thin women get PCOS?
Absolutely. This is known as “Lean PCOS.” While they may not have the same weight struggles, their genetics still cause androgen excess and ovulation issues, often triggered by stress or inflammation rather than just insulin.
Is PCOS an autoimmune disease?
Not exactly. While it involves chronic inflammation and an overactive immune response, it isn’t classified as a classic autoimmune disease. However, many women with PCOS also have autoimmune issues like Hashimoto’s Thyroiditis.
Can PCOS skip a generation?
Yes. Because it requires environmental triggers, your mother might have carried the genes but lived a lifestyle that kept them silent, while you encountered a trigger that activated them.
Does trauma trigger PCOS?
Significant emotional or physical trauma spikes cortisol levels. For those with a genetic predisposition, this intense stress can be the “pull” on the trigger that starts the hormonal cascade of PCOS.
Final Takeaway: PCOS Is Genetic—But It’s Not Destiny
Your DNA is a map, but you are the driver. Knowing that PCOS is genetic should be a source of relief, not despair. It means your struggles aren’t due to a lack of willpower; they are a biological reality.
In 2026, we have more tools than ever to “silence” these genes. By managing your insulin, protecting your sleep, and reducing your toxic load, you can lead a vibrant, healthy life where PCOS is just a background note, not the lead singer of your story.
📚 References
- International evidence-based guideline for the assessment and management of polycystic ovary syndrome.
Human Reproduction, 33(9), 1602–1618.
https://academic.oup.com/humrep/article/33/9/1602/5056069
- Diagnosis and treatment of polycystic ovary syndrome: An Endocrine Society clinical practice guideline.
Journal of Clinical Endocrinology & Metabolism, 98(12), 4565–4592.
https://academic.oup.com/jcem/article/98/12/4565/2836069
- The role of genes and environment in the etiology of PCOS.
Endocrine, 30(1), 19–26.
https://pubmed.ncbi.nlm.nih.gov/17185788/
- Polycystic ovary syndrome: Etiology, pathogenesis and diagnosis.
Nature Reviews Endocrinology, 7(4), 219–231.
https://www.nature.com/articles/nrendo.2010.217
- The pathogenesis of polycystic ovary syndrome (PCOS): The hypothesis of PCOS as functional ovarian hyperandrogenism revisited.
Endocrine Reviews, 37(5), 467–520.
https://academic.oup.com/edrv/article/37/5/467/2354709
- National Institute of Child Health and Human Development (NICHD).
What causes PCOS?
https://www.nichd.nih.gov/health/topics/pcos/conditioninfo/causes
- MedlinePlus (U.S. National Library of Medicine).
Polycystic ovary syndrome.
https://medlineplus.gov/polycysticovarysyndrome.html



